Understanding Pediatric Eczema in Newborns & Children
Atopic dermatitis, a type of eczema, is a common chronic skin condition in infants and children. It often starts in the first few months of life and can worsen or change as children grow. Symptoms are more common and may be more severe in children with skin of color.

Eczema can make a child’s skin become very dry, irritated, itchy, and inflamed. The symptoms can make them feel uncomfortable and keep them awake at night.
Eczema can cause short-term flare-ups and long-term changes to the appearance of the skin. Contrary to popular belief, it does not go away in all children. Eczema may become milder or flare less often as some children age. With the right skin care routine and treatment, many babies and children get better from eczema as they grow.
Talk with your child’s pediatrician or an eczema specialist, such as a board-certified allergist and immunologist or a dermatologist, to develop an age-appropriate treatment and management plan.

Causes and risk factors of pediatric eczema
Some children are more likely to get eczema because it can run in families. The skin condition may be triggered by environmental factors, such as allergens or the weather. Even as children grow, their skin remains more sensitive than those who do not have eczema. An eczema flare-up can happen at any stage of life. It can go away for a while and come back.
The most common reasons for eczema in children include:
Family history. Children are more likely to have eczema if their family members have eczema, asthma, or allergies. They may inherit traits that make their skin lose moisture more easily and become dry and irritated.
Weak skin barrier. The skin barrier helps keep moisture in and protects against germs and irritants. When this barrier is weak, it is easier for the skin to get dry, itchy, or inflamed.
- Baby’s skin barrier (0–1 year). Thinner than adult skin. It loses water fast and can let germs in more easily. Babies make less oil, so their skin dries out. Sweat glands are still growing.
- Child’s skin barrier. Between ages 2 and 5, the barrier gets stronger but can still be sensitive. Moving and sweating can irritate it.
- Teen skin barrier. Hormones cause the skin to produce more oil. Skin may get greasy or break out. Acne creams, makeup, or shaving can dry or upset the skin and trigger eczema.
Environmental triggers. Things at home or outside can irritate a baby’s skin and cause eczema. Common eczema triggers include:
- Harsh soaps, detergents, and fragrances can remove natural oils, leaving the skin extra dry.
- Skin care products with plant oils or other plant-based products can irritate the skin.
- Fabrics like wool, polyester, Spandex or tight, rough clothing can rub against the skin and make it even more irritated. These fabrics can also trap heat against the skin, increasing the risk of an eczema flare.
- Changes in the weather, temperature, or humidity can cause the skin to lose moisture, which may lead to flare-ups.
- Environmental allergens like pollen, mold, dust mites and pet dander can contribute to eczema flares.
- Overheating or sweating makes itching and redness worse and can lead to eczema symptoms.
Some parents feel their child’s flares are caused by certain foods. While foods may sometimes trigger symptoms, they do not cause eczema. Babies with eczema are at higher risk of developing food allergies.
If you are concerned about foods causing your child’s eczema, keep a food journal and track symptoms and triggers. Do not eliminate any foods from your child’s diet without first discussing this with a doctor. Avoiding foods can actually cause a food allergy to develop. It can also affect your child’s nutrition and growth.longside a trained healthcare provider. Food avoidance can actually lead to a food allergy.

Preventing eczema in children
While eczema can’t always be prevented, there are steps that may help protect your child’s skin and lower the risk of flare-ups:
- Moisturize early. If your baby has family members with skin problems or allergies, use a scent-free cream to moisturize the skin every day, especially after bathing. This might help keep your baby’s skin from drying out. It could also lower their chance of getting eczema.
- Gentle skincare. Avoid harsh soaps, bubble baths, and products with strong fragrances. Choose mild cleansers and gently pat-dry your child with a soft towel after bathing.
- Early food introduction. For some children with severe eczema, introducing peanut and egg around 4–6 months may help reduce the risk of developing food allergies. Always talk with your child’s pediatrician before starting new foods.
- Dress for comfort. Use soft, breathable cotton clothing that is loose-fitting. Avoid synthetic fibers like polyesters, spandex and wool blends.
- Keep skin cool. Avoid overheating. Sweating can trigger itching and eczema flare-ups.
Even if eczema develops, these steps can help reduce how severe it becomes. Follow this skin care routine early in infancy and continue it daily for best results.

Eczema symptoms in children
Knowing the symptoms of eczema early is important for care. Atopic dermatitis in children often starts with mild skin irritation but can become severe if not treated. Typical symptoms of atopic dermatitis include:
- Dry, itchy patches: A dry, itchy skin rash that may be rough, scaly or flaky to the touch. Children often rub or scratch these areas. This can irritate the skin even more, leading to additional skin problems.
- Eczema rash: Red or dark patches on the skin can appear. In darker skin tones, the rash may look purple, brown or gray. If not treated quickly, thickened skin can develop. Repeat scratching can also lead to lightening or darkening of your child’s normal skin tone.
- Bumpy skin: Babies and children with darker skin tones may have several tiny bumps with or without redness and darker areas of skin. This is called follicular accentuation and is a sign of eczema.
- Oozing, crusty skin: Broken skin can let in germs, causing crusting or oozing. Getting help early from your doctor can decrease the risk of infections.
While eczema can look different depending on your child’s age, common signs include dry, itchy, and inflamed patches. Below are some age-specific examples.
What does atopic dermatitis look like in babies?
In the first year of life, eczema often starts on the face and can spread to other parts of the body as babies grow and begin to crawl. It is important to check all areas for irritated or thickened skin. Eczema usually does not appear in the diaper area because it stays moist, but irritation can still happen if there is friction or contact with soaps and wipes. Common locations and signs include:
Newborns (0–6 months):
- Cheeks, chin, forehead and neck folds
- Back of the arms, inner forearms, elbows, wrist creases and hands
- Legs, creases behind knees, ankles and the top of the feet
- Skin texture can be thicker in inflamed skin
- Skin color may range from pink, red, purple, gray or dark depending on skin tone
Babies (6–12 months):
- Elbows and knees (especially from crawling)
- Hands and feet
- Face (especially on the cheeks and around the eyes and mouth)
- Dry or irritated patches where the skin rubs against surfaces
- Skin texture can be thicker in inflamed skin
- Skin color may range from pink, red, purple, gray or dark depending on skin tone
What does atopic dermatitis look like in toddlers?
In toddlers, eczema often becomes more concentrated in the skin folds (flexural areas) as babies become more mobile. Common locations and signs include:
- Inside the elbows and behind the knees
- Wrists and ankles
- Neck creases
- Around the mouth from pacifier rubbing and drool, with possible thickened patches from frequent scratching
- Skin texture can be thicker in inflamed skin
- Skin color may range from pink, red, purple, gray or dark depending on skin tone
What does eczema look like in older children?
As children grow older, eczema often becomes chronic and thicker, especially in areas frequently rubbed or scratched. Typical signs and locations include:
- Thick, leathery patches from repeated scratching known as lichenified plaques
- Dry, scaly patches on the backs of the knees, inside elbows, neck, hands, wrists and ankles
- Hand eczema often comes from hand washing and contact with irritants. This looks like dry, cracked skin on the palms and fingers.
- Post-inflammatory color changes. These are darker or lighter patches that last even when the eczema calms down.
What does eczema look like in teens?
In teenagers, eczema often becomes more chronic and stubborn. It can show up in many of the same places as in younger children, but flare-ups may last longer or come back more often. Hormonal changes, stress, and new skincare or makeup products can also trigger symptoms. Common locations and signs include:
- Thick, dry patches on the hands, wrists, elbows, and behind the knees
- Dry, scaly skin on the neck and around the eyes
- Areas of redness or darker patches (purple, brown, or gray depending on skin tone)
- Rough or leathery skin from frequent scratching (lichenification)
- Hand eczema, especially if your teen washes hands often or uses irritating products

Diagnosing eczema in children
Doctors diagnose eczema by first checking the skin. They look for dry skin and bumpy, irritated or itchy spots and try to identify a pattern of skin changes. Doctors also make sure symptoms are not something else, such as a skin infection or other rashes that can look like eczema.
Doctors will ask about the family’s health and what might trigger the rash. It may be helpful to keep a detailed diary of symptoms: where the rash occurs, what makes it better or worse, and products used on the skin (such as wipes, moisturizers, body washes, sunscreen or makeup). This can help doctors pinpoint what’s causing the eczema. It can also help diagnose eczema.
Here are some tips to help with the diagnosis:
- Spot the differences: You might see spots that are itchy or feel thicker. This may be the only sign of eczema in children with darker skin. The spots may indicate areas of the skin that need management.
- Take photos: Take pictures of flare-ups. These photos can show how the skin looks when the eczema is active and when it calms down. They help the doctor see changes over time.
- Find the right doctor: Your child’s pediatrician will be able to provide appropriate care, but you can also seek out a specialist, such as an allergist or dermatologist who has experience treating all skin tones.

Treating eczema in children and infants with skin of color
Since eczema is a chronic or long-term problem for the skin, treating eczema requires a consistent routine to always be protecting and restoring the skin barrier. This means taking care of skin every day to keep it moisturized and calm. What to do if daily care isn’t enough? Your child’s healthcare provider may recommend creams, ointments or other medications to stop inflammation and ease itching.
Moisturizers should be part of your child’s skin care routine for eczema. They help protect the outer layer of the skin by:
- sealing in moisture
- combating dryness and scaly skin
- keeping out allergens, irritants and bacteria
- soothing the skin for long-lasting hydration
- preventing flare-ups
It’s recommended you apply a moisturizer to your child at least twice per day, including once after a bath or shower. Develop a schedule so that moisturizing becomes part of a skincare routine to keep your baby’s skin hydrated.
Medications used for treating eczema:
- Topical corticosteroids: Reduce inflammation and itching. Strength of the cream or ointment depends on the severity and body area. Prolonged use, especially of stronger steroids, can sometimes lighten skin color or thin the skin.
- Non-steroidal topical creams: Calcineurin inhibitors (Elidel®-pimecrolimus, Protopic®-tacrolimus), topical JAK inhibitors (Opzelura®-ruxolitinib, Anzupgo®-delgocitinib), aryl hydrobarbon (VTAMA® – tapinarof) or PDE4 inhibitors (Eucrisa®-crisaborole or Zoryve®-roflumilast) help control inflammation without steroids. These are approved for various ages. Some creams may cause stinging or burning when first used, but this usually improves with continued use.
- Oral antihistamines: Sometimes used to help control nighttime itching. They don’t treat eczema itself, but can help with sleep. Oral antihistamines are not meant to be used long-term to control itching, however.
- Biologics: These are injectable medicines that target pathways of the immune system to help heal the skin from the inside out. They are usually prescribed for moderate-to-severe symptoms. One of the available biologics can be prescribed for babies as young as 6 months of age. Doctors usually recommend biologics when other treatments don’t work well or if your child has severe, hard-to-control eczema. These biologics include tralokinumab (Adbry®), dupilumab (Dupixent®), lebrikizumab (Ebglyss®) and nemolizumab (Nemluvio®).
- Oral JAK inhibitors: These come as pills or liquid solutions to help control inflammation and reduce chronic eczema flare-ups. They include abrocitinib (Cibinqo®) and upadacitinib (Rinvoq®). Oral JAK inhibitors are usually prescribed for older children or teens when other treatments have not worked. The medications require careful monitoring by a doctor.

Other ways to manage pediatric eczema
If your child’s eczema does not get better with usual care, your doctor may suggest one or more of these treatments.
Phototherapy (light therapy): This treatment uses controlled UV light in a clinic to help calm severe eczema. It is usually for older children or teens whose eczema does not get better with creams.
Wet wrap therapy: Wet wraps can be used for babies, toddlers, and older children during severe eczema flares. This treatment involves putting moisturizer or medicine on the skin, then covering it with damp bandages or clothing and a dry layer on top. Wet wraps help calm itching, reduce redness, and promote skin healing. Always ask your doctor to show you how to do wet wraps safely, especially for infants, since their skin can absorb medicine more easily.
Antimicrobial treatments and bleach baths: Children with eczema often have more bacteria on their skin. This can cause infections or make eczema worse. Doctors sometimes recommend bleach baths or antiseptic washes to help. A bleach bath (sometimes called a swimming pool bath) uses a small amount of bleach diluted in a full tub of water, similar to swimming in a chlorinated pool. Bleach baths are safe for babies and children of all skin colors when used as directed. They do not lighten the skin but can help reduce germs and prevent flare-ups. Always follow your doctor’s instructions and apply moisturizer right after the bath to keep skin soft.
Eczema treatment considerations by age
Children of different ages may need different treatment plans because their skin absorbs medicine differently, and some treatments are safer for certain ages.
| Age Group | Topical Medications | Other Treatments & Considerations |
|---|---|---|
Infants (0–12 months) |
|
|
Toddlers (1–3 years) |
|
|
Children (4–11 years) |
|
|
Teens (12–18 years) |
|
|
Many parents worry about using steroid creams on their child’s skin. But when used the right way, with a doctor carefully monitoring for appropriate doses and frequency, these medicines are safe and can help prevent worse problems later. Not treating bad flares can lead to more itching, infections, and thick, damaged skin over time.
Always follow your doctor’s direction about how much and how often to use steroid creams. A good rule for how much to use is 1 fingertip unit (from the tip to the first knuckle) for a palm-sized body surface area.

Managing your child’s eczema day to day
Taking care of eczema requires daily routines and smart choices at home. These habits help keep your child’s skin calm, manage symptoms, and prevent flare-ups. As children grow, their needs will change, so it helps to adjust your approach over time.
Daily care basics for eczema:
Moisturizing
- Keep skin hydrated with fragrance-free creams or petroleum jelly.
- Apply moisturizer at least twice a day, especially right after a bath, to lock in moisture.
- Use fragrance-free mineral sunscreen (zinc oxide or titanium dioxide) on exposed skin if your child is outdoors. Test on a small area first to check for irritation.
Bathing
- Keep baths or showers short. Use lukewarm water.
- Use a gentle cleanser or soap-free wash.
- Avoid hot water, rough washcloths, and products with strong scents.
- Gently pat skin dry and moisturize right away.
Environment and Triggers
- Keep your home at a mild temperature and 30–50% humidity to protect the skin barrier.
- Use gentle, fragrance-free soaps and cleaning detergents.
- Try to limit exposure to common triggers like dust mites, pet dander, and pollen.
- Use a HEPA air filter if environmental allergens are a trigger.
- Keep windows closed during high pollen seasons.
- Wash bedding in hot water weekly to reduce dust mites.
- Vacuum carpets and furniture often.
Clothing
- Dress your child in soft cotton layers.
- Avoid wool and scratchy fabrics.
- Use mittens or bodysuits at night to help prevent scratching.
Food Allergies
- Only avoid foods if your child has been diagnosed with a food allergy. Some families may worry that certain foods are contributing to eczema. Discuss these concerns with your doctor.
- Talk to your child’s allergist before removing any foods. Avoiding foods or removing foods from the diet without medical advice can increase the risk of developing a food allergy. Younger children are at higher risk of developing allergy due to food avoidance.
- New research shows that early introduction of peanut and egg between 4–6 months of age may help prevent food allergies if your baby has eczema. All infants should have common food allergens introduced in the first year of life. (Food allergy testing is not required prior to introduction.)
Watch for skin infections
Eczema can cause the skin to crack, making it easier for bacteria to enter. Spotting the early signs of infection is important to prevent it from getting worse. If you notice any worrying symptoms, contact your doctor. Signs of infection include:
- Yellow crusts or oozing fluid.
- Skin that appears very sore, swollen, or warm.
- Fever or a sudden worsening of symptoms.
Doctor Visits
- Regular check-ins with your child’s pediatrician, allergist or dermatologist are important to see how treatments are working and adjust as needed.
Eczema management changes with age
Below are tips for each stage:
Eczema management tips for infants (0–12 months)
- Bathing: Daily lukewarm baths, gentle cleanser, fragrance-free moisturizer after.
- Moisturizing: 2–3 times per day.
- Clothing: Soft cotton layers. Cover hands if needed to prevent scratching.
- Wipes and diaper care: Choose fragrance-free baby wipes without alcohol or harsh chemicals. Pat (don’t rub) the skin dry.
- Surfaces: Clean changing tables, play mats, and crib sheets with gentle, unscented cleaners to avoid irritation from residues.
- Early Food Introduction: If your baby has eczema, talk to your pediatrician about the importance of introducing the top allergens starting around 4 to 6 months. Early, regular introduction may help lower the risk of developing food allergies.
Eczema management tips for toddlers (1–3 years)
- Teaching gentle habits: Help your child learn not to scratch. Try distractions or soft mittens.
- Moisturizing: Make it part of the daily routine. Let them “help” apply cream to build a positive habit.
- Sleep: Keep the bedroom cool and use cotton sleepwear.
- Triggers: Watch for friction from crawling, drooling, or rough fabrics.
- Feeding time: Use a soft bib or cloth to protect the skin around the mouth and neck when eating. Gently clean off food right after meals to prevent irritation.
Eczema management tips for school-aged children (4–12 years)
- Daily routine: Moisturize before school and at bedtime.
- Sports: Rinse off sweat off right after activity and reapply moisturizer.
- Independence: Teach your child to know the signs of early itching and to use creams on their own.
- Stress and itching: Offer fidget toys or other tools to keep hands busy.
- School: Talk with teachers about eczema, needed accommodations, and medication plans.
- Peers: Discuss self-confidence and ways to handle teasing or questions from classmates.
- Sleep: If nighttime itching is affecting school, ask your doctor for strategies to help improve sleep.
Eczema management tips for teens (13–18 years)
- Daily routine: Keep moisturizing a daily habit, morning and night. Teens can keep a small tube of cream in their backpack or locker. Patch-test new products like makeup and deodorants.
- Stress and mental health: Stress and anxiety can trigger flares. Encourage stress-relief habits like exercise, deep breathing, or journaling. If your teen feels down or embarrassed about their skin, a counselor or support group can help build confidence.
- Independence: Involve them in appointments so they feel a sense of ownership over their care plan.
- Activities: After sports or workouts, teens should shower and moisturize right away to remove sweat. Choose soft, breathable clothing for exercise.
- Social life: Talk openly about self-esteem, dating, and peer pressure. Eczema doesn’t define who they are.
Eczema co-morbidities in children
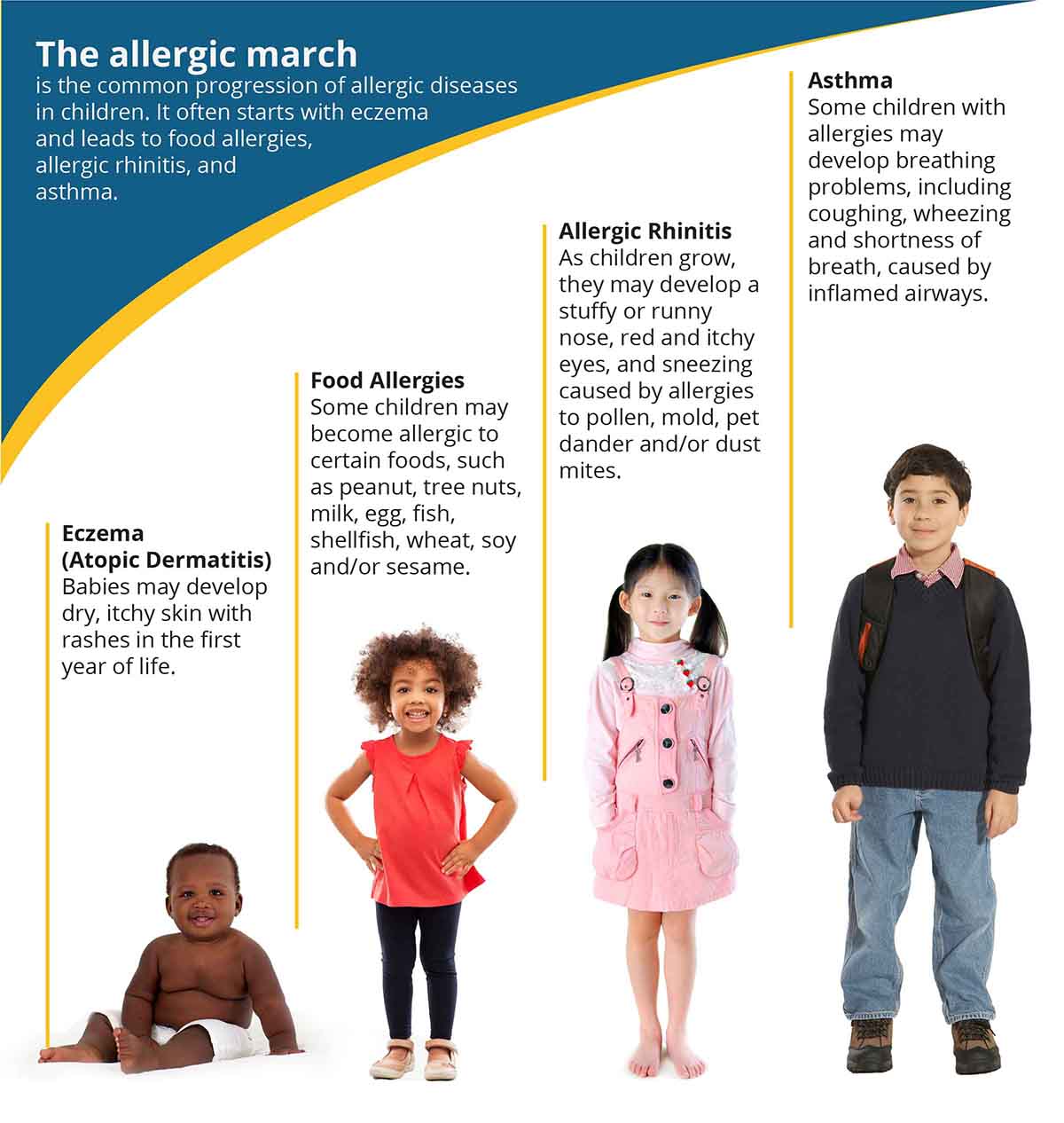
Eczema is sometimes linked to other health conditions (called co-morbidities). These health problems may include asthma and environmental allergies. Co-morbidities can develop one after another in a pattern called the atopic march (also called allergic march).
The atopic march often starts with eczema in infancy or early childhood. As children grow, some may also develop food allergies, allergic rhinitis (hay fever), or asthma. Not every child with eczema will have these conditions, but it is important to watch for symptoms. Early care and treatment can help lessen the impact on your child’s health.
Food allergies
Some children with eczema also have food allergies. This means their body reacts to foods like nuts, dairy or eggs. Food allergy reactions are different from eczema flares. Some food allergy symptoms may include:
- Hives or swelling
- Stomach pain or vomiting
- Breathing problems
- Difficulty breathing
- Swelling of the tongue or throat
- Dizziness or fainting
Food allergy reactions can be mild or serious and happen within minutes or a few hours after eating the food. Always talk to your child’s doctor if you think your child has a food allergy, as some reactions can be serious. Severe allergic reactions are called anaphylaxis. Talk to your allergist about food allergy testing and making a plan to keep your child safe.
Allergic rhinitis (environmental allergies)
As children grow older, they may develop allergy symptoms when exposed to pollen, dust mites, or pets. These include:
- Sneezing
- Runny or stuffy nose
- Itchy, watery eyes
Asthma
Eczema can sometimes be an early sign in a chain of allergic conditions that lead to asthma. Asthma symptoms may appear later in childhood and can include:
- Wheezing or coughing
- Shortness of breath
- Tightness in the chest
Remember, not all children with eczema will go on to develop these other conditions. Regular check-ups with your child’s pediatrician or allergist can help you watch for symptoms and get the right care early. Allergists are specialists in treating asthma as well as allergies and eczema.
Other factors that may impact skin health
There are a few other key factors that can affect eczema in children:
- Skin infections. It is not uncommon to have broken or cracked skin, which makes it easier for bacteria or germs to get into the body. Watch for yellow crusting, discharge or pus, or sudden worsening. These may be signs of infection.
- Sleep problems. Itching can disturb sleep and make your child cranky or distracted. Ask a doctor about safe ways to lessen nighttime scratching, such as soothing baths, gentle moisturizers or topical medications. Oral antihistamines that are sedating (cause drowsiness) may help reduce itching so your child can get to sleep. But keep in mind that oral antihistamines do not treat eczema.
- Emotional and social effects: Severe eczema flares can be stressful for infants and children, family members and caregivers. Stress can also trigger eczema flares. Talk to a healthcare provider or counselor if stress becomes overwhelming.

Social, emotional, and academic impacts of eczema
Children, adolescents and teenagers with eczema often face extra challenges that can affect their confidence, friendships, and learning:
- Bullying or teasing: Visible rashes can lead to comments or feeling left out.
- Self-esteem and body image: Kids and teens may feel embarrassed or self-conscious about their skin, especially in social or dating situations.
- Peer pressure: Worrying about fitting in or explaining eczema to friends can be stressful.
- Sleep disruption: Itching at night can make it harder to focus and learn.
- School participation: Some children with asthma may avoid gym, swimming, or field trips when symptoms are flaring.
- Independence: Children and teens often need help learning how to manage treatments. Older kids may want more privacy as they get older.
- Mental health: Anxiety and depression are more common in kids and teens with chronic eczema.
Tips for caregivers:
- Encourage open conversations about feelings, stress, and worries.
- Praise your child or teen when they practice good self-care or cope with challenges.
- Role-play or discuss how to respond if other kids ask about eczema.
- Talk with teachers about any needed accommodations, like extra time to apply moisturizers or taking breaks during flare-ups.
- Create an “eczema kit” with creams, bandages, and wipes to bring to school or activities.
- If your child or teen feels anxious or sad about their skin, consider a counselor.
- Find a support group – in person or online – that involves adolescents and/or teens.
- Remind them that eczema doesn’t define who they are.
Questions & answers (Q&A) on pediatric eczema
Below are some frequently asked questions about pediatric eczema. It is also referred to as atopic dermatitis, infant eczema or baby eczema, and sometimes mistakenly called “atopic eczema.”



